ARTERY SURGERY
We have seen significant steps forward in the treatment of coronary artery disease over the last few years, both in the field of angioplasty and surgery.
CORONARY ARTERY SURGERY:
Coronary artery surgery in turn has made advances over the last few years as follows:
1- Technical advances:
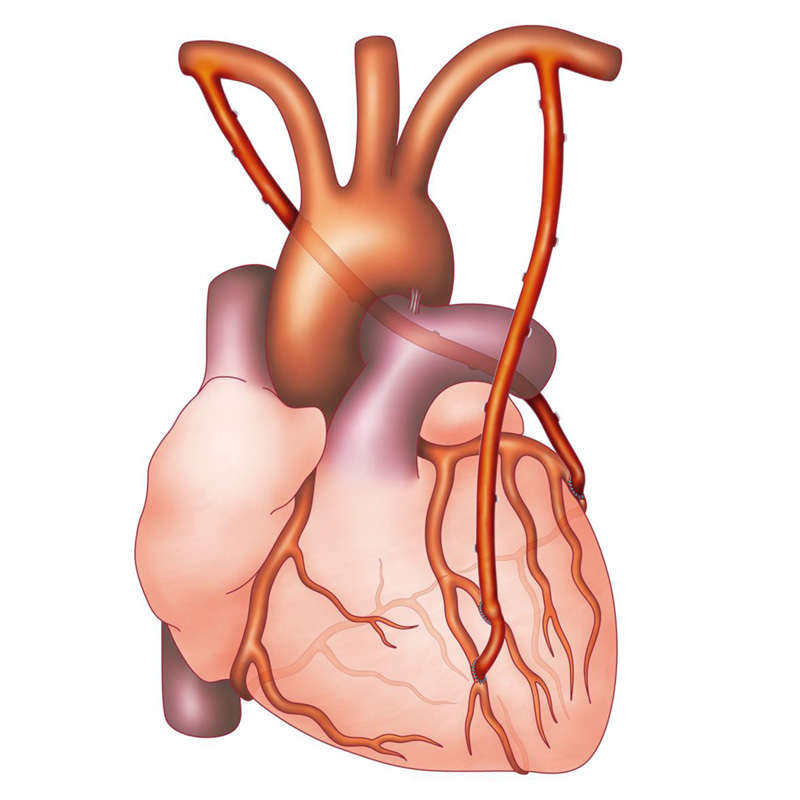
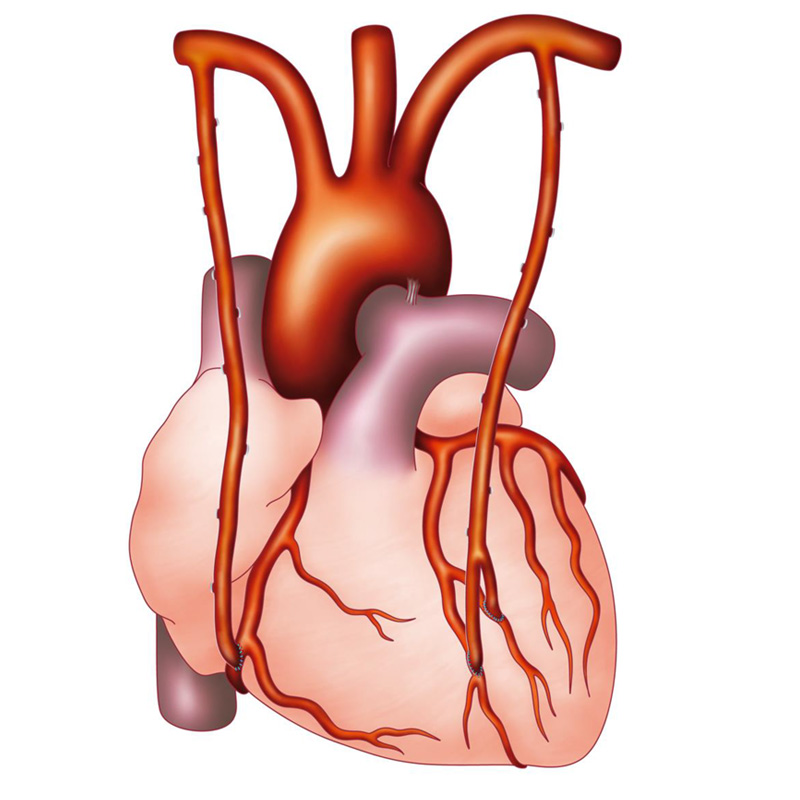
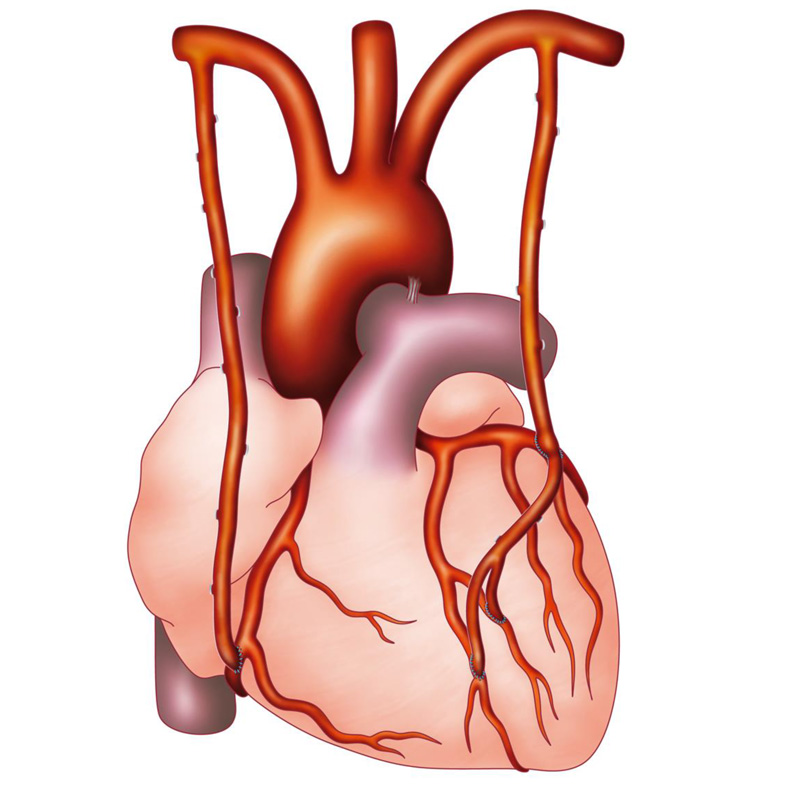
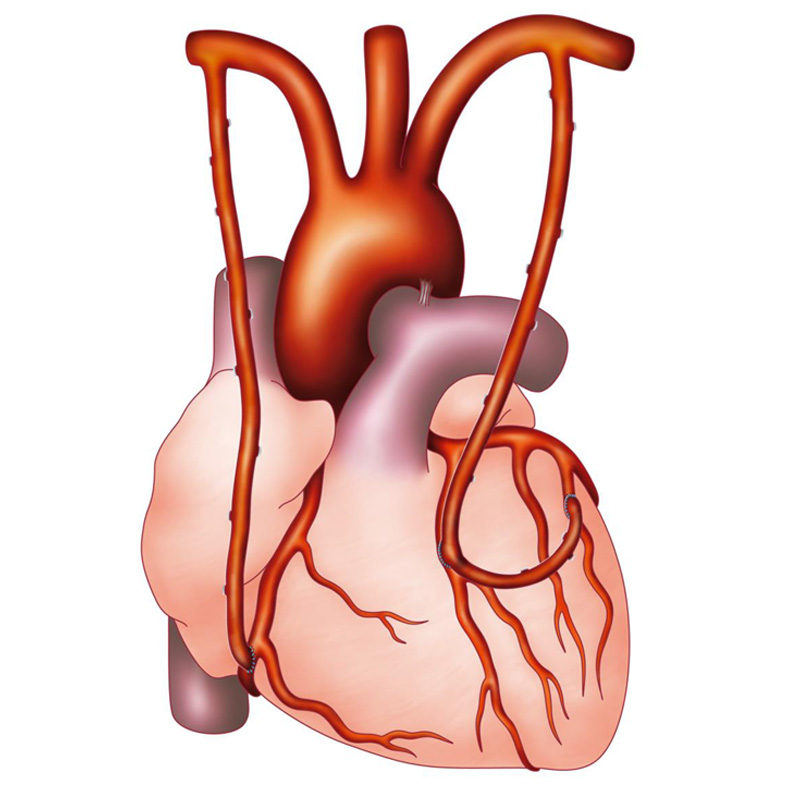
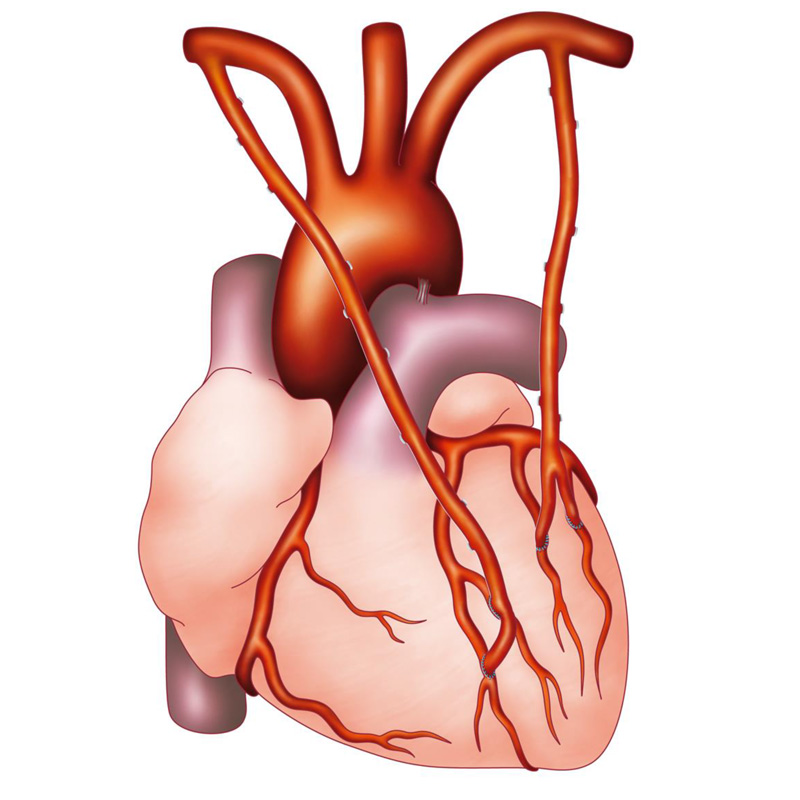
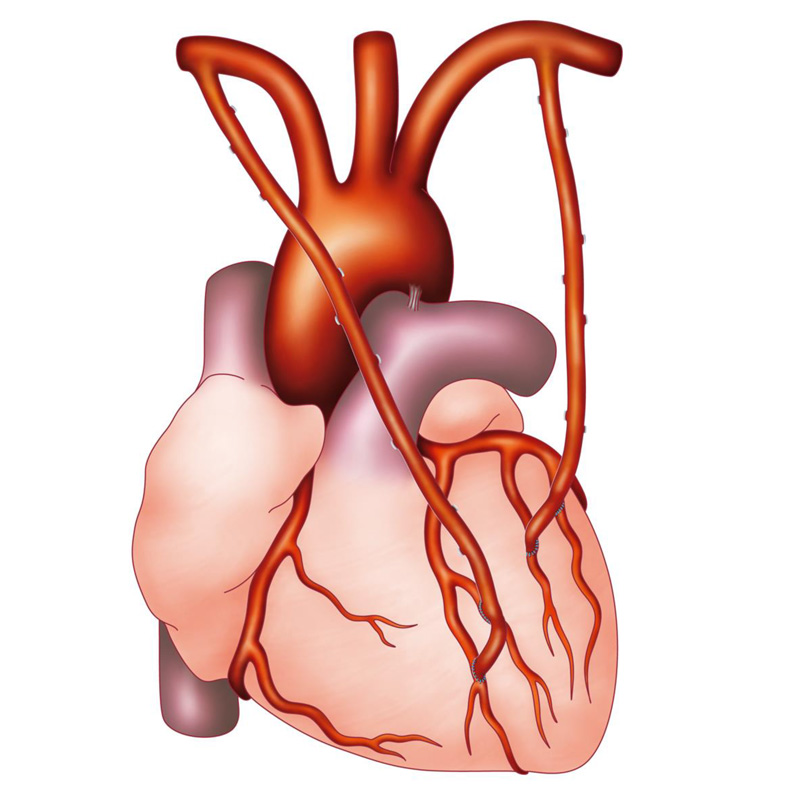
Systematic use of 2 mammary artery grafts (Total arterial coronary bypass).
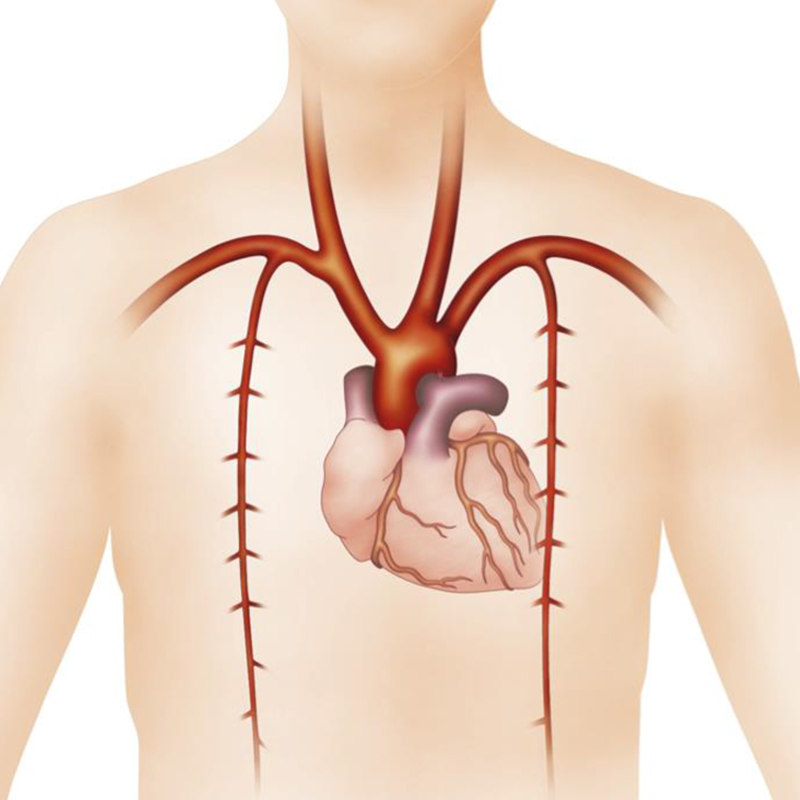
The 2 Internal Mammary Arteries are two excellent arterial grafts, whose anatomical structure and calibre are identical to that of the coronary arteries. This accounts for their longevity in comparison to other types of grafts: veins, radial artery…
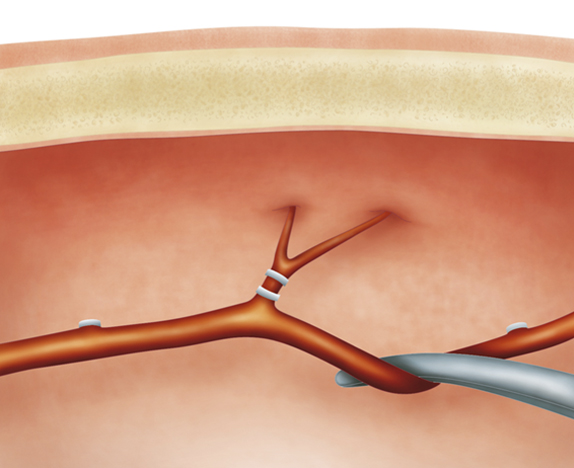
For Pr Khoury and according to his experience, the two “pediculated” internal mammary artery grafts (i.e., not sectioned, used as a free graft or as a “Y” graft) make it possible to perform, in almost all cases, a so-called complete and “Anatomical” revascularisation. This also takes into account anatomical variations by favouring the dominant coronary artery network and the patient’s coronary artery lesions.
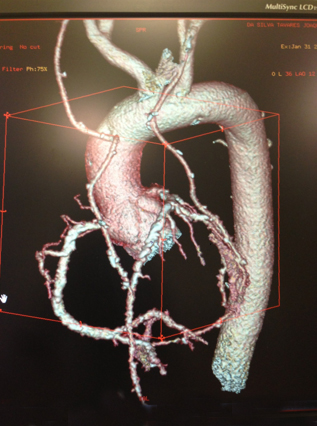
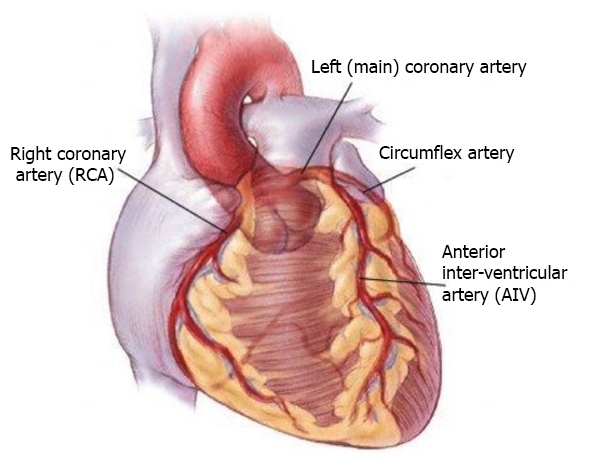
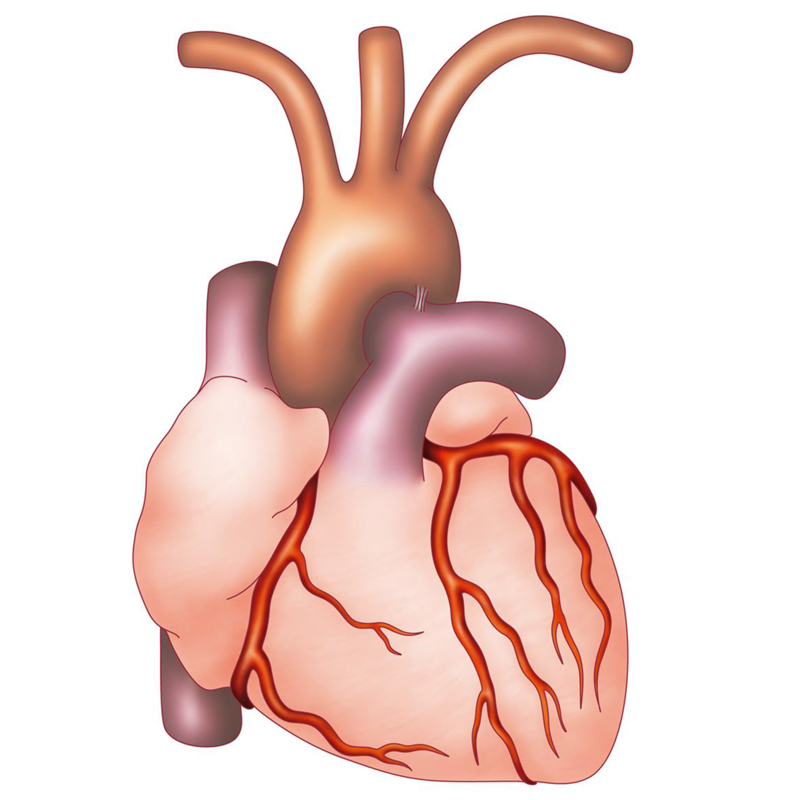
The diagrams above show us the different possibilities.
See article “Anatomic coronary revascularisation” and the link.