SURGERY
Congenital heart disease :
The Laënnec-Necker hospital centre is one of the largest facilities world-wide and renowned for paediatric cardiac surgery for the diagnosis and treatment of congenital heart defects.
This is where Dr. Wassim Khoury has spent most of his medical training and acquired his experience in this field.
It is also in this centre that humanitarian missions are organised and sent to countries where there is a need for them.
Dr. Wassim Khoury summarised this experience in a textbook detailing surgical techniques for these disorders and in a speciality which is making major advances.


SURGICAL TECHNIQUES
Tetralogy of Fallot
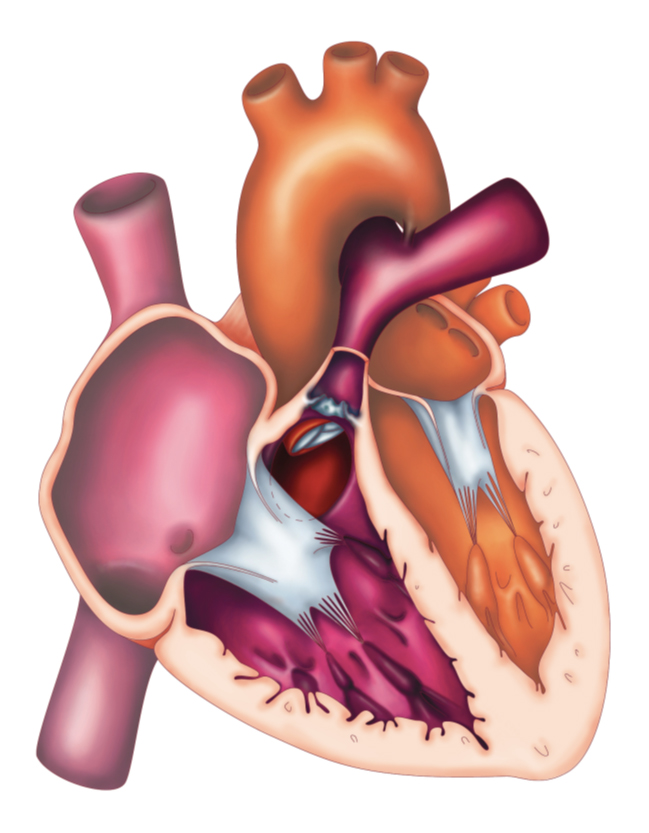
Anatomical description
Accounting for 10% of congenital heart disease cases, the Tetralogy of Fallot remains the most common cyanotic cardiac malformation in children.
An anomaly first described by French physician Arthur Fallot in 1888; Fallot’s Tetralogy consists of four anomalies:
-
A large Ventricular septal defect (VSD).
-
Pulmonary artery stenosis (infundibular) together with valvular stenosis.
-
Aortic dextroposition, in which the aorta is displaced rightward overriding the VSD.
-
Right ventricular hypertrophy.
The aortic arch may be located on the right side in about 25% of cases and intra-atrial communication may also exist in a third of patients.
Fallot’s Tetralogy consists of several degrees of severity. The more severe the right artery stenosis is, the more the left-right shunt increases, resulting in cyanosis.
Severe hypoplasia of the pulmonary artery branches, the existence of multiple VSD, with coronary artery anomaly, can delay complete recovery by making the surgery more difficult or such that it has to be performed in two stages (use of a valvular tube, residual VSD, etc.).
Technique chirurgicale
The timing chosen for a complete surgical procedure is not fixed.
At birth, severe cyanosis requires use of an infusion of Prostaglandin E1, to maintain the ductus arteriosus open and pulmonary blood flow.
In some selected cases, palliative treatment with Blalock-Taussig shunt, can be offered (hyper-cyanotic malaise), making it possible to restore pulmonary blood flow.
Complete surgical cure, requires extra-corporeal circulation (ECC) and clamping of the aorta. It is indicated theoretically between 4-6 months of age and, depending on the progression of cyanosis, it can be performed at a more or less early age.
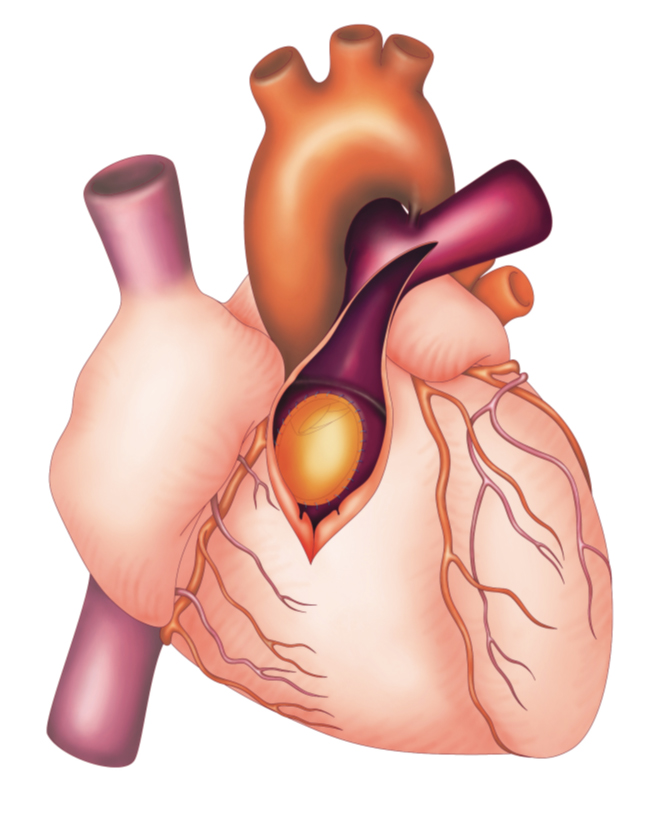
Technically, repair consists of:
-
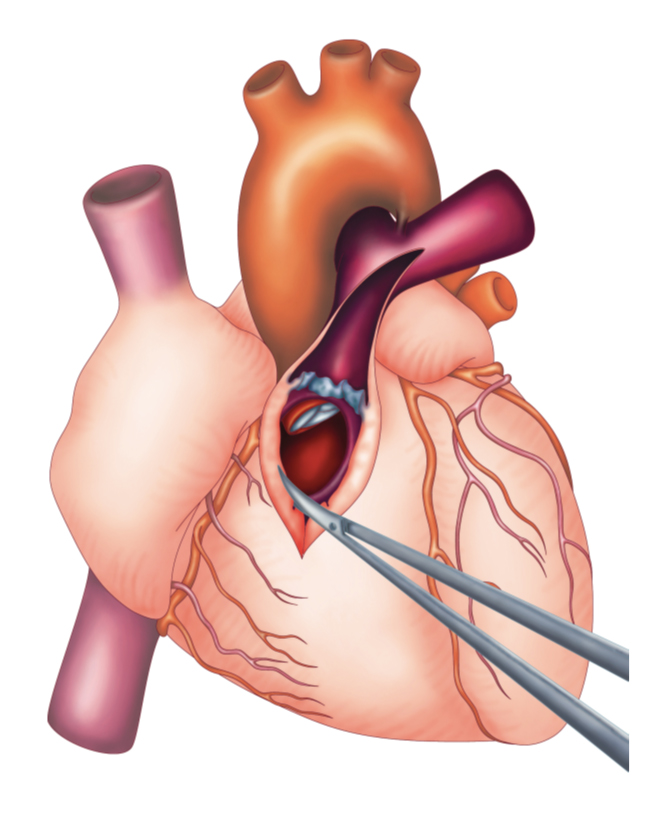
Closure of the VSD
-
Unblocking of the right pulmonary artery branches
Two approaches are possible:
Repair via the right atrium or by right ventriculotomy.
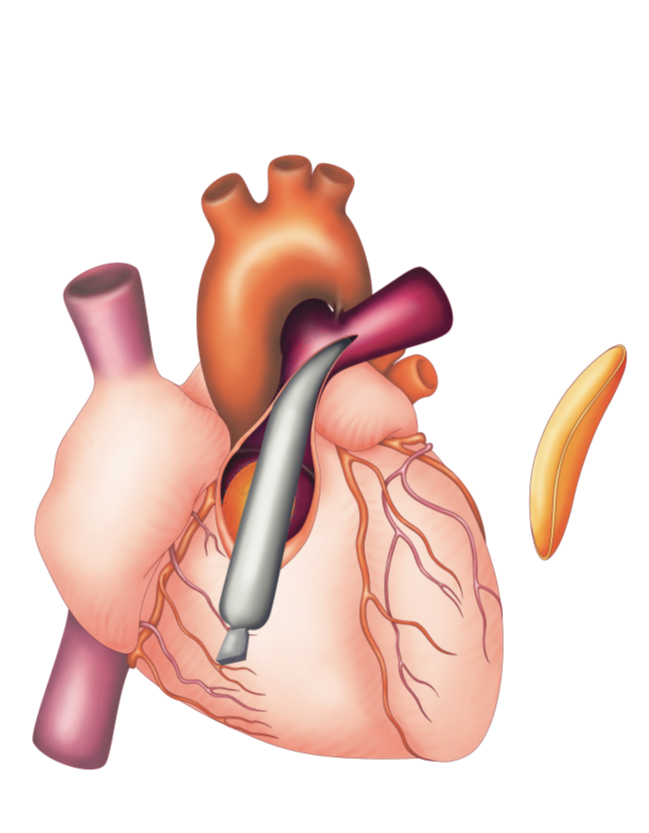
Depending on degree of obstruction of the ejection pathway, the former is removed first, by resection of obstructing muscle. Then, closure of the VSD with a patch of pericardium conserved and fastened with separate sutures (see diagram no.).
Widening and reconstruction of the right vessels is then performed as required, calibrated by Hégar dilators using a reference table and taking body weight into account (see table…)
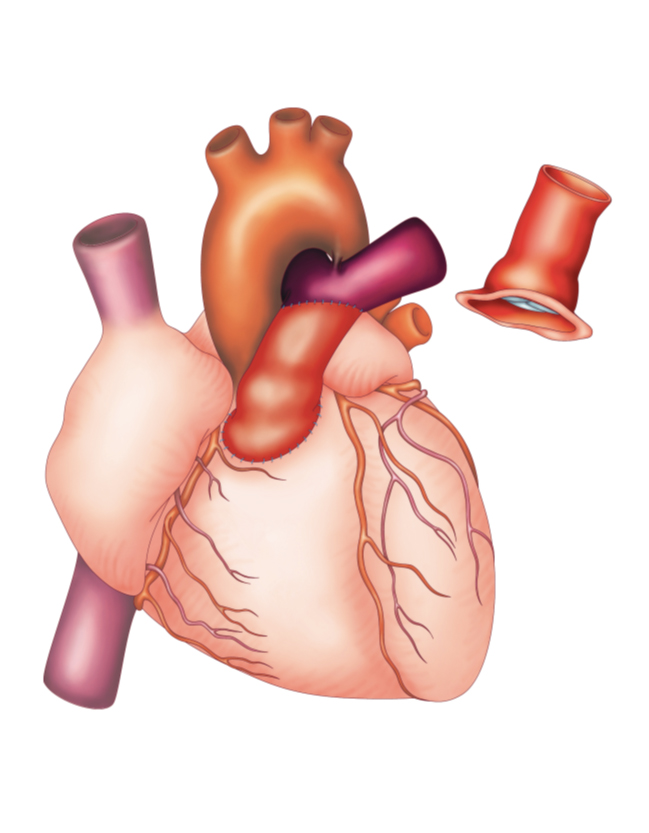
Naturally, preservation of the pulmonary ring and valve must be attempted whenever possible making it possible to maintain a competent pulmonary valve.
A trans-annual patch is often necessary to obtain adequate reconstitution of the right artery branches (see diagramme below).
After unclamping the aorta and removing the ECC, measurement of pressure in the right ventricle and/or transoesophageal echocardiography make it possible to access the repair. Generally, duration of clamping of the aorta and of the ECC are moderate.
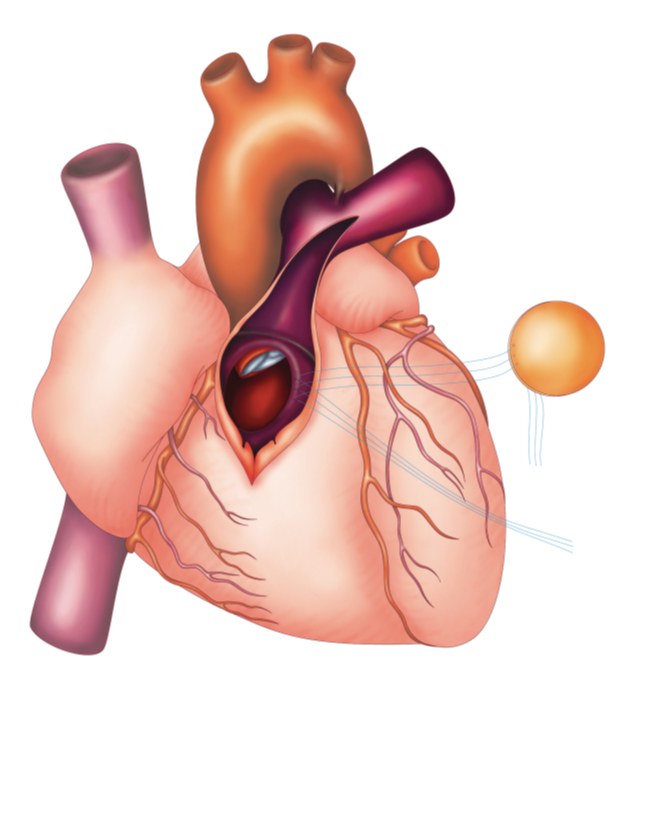
Fermeture de la civ